16-year old girl with complaints of high-grade fever, bilateral knee joints pain and skin rash
By: Medcase Editor

16-year old girl with complaints of high-grade fever, bilateral knee joints pain and skin rash Overview
- Presenting Complaint
- Patient History
- Review of Systems
- Physical Examination
- Diagnostic Test
- Diagnostic Imaging
- Diagnosis and Management
- Discussion
A 16-year old girl with complaints of high-grade fever, chest pain, SOB , and bilateral knee joints pain and rash over the arms/legs for 1 week
Visit our partner site
- History of presenting
- Past Medical/Social hoistory
- Past surgical history
- Family history
- Current Medication
She also denied pain abdomen, vomiting, loose stools or burning sensation during micturition.
no petechial spots or history of pruritus
General
Heent
Neck
Cardiovascular
Lungs
Abdomen
Extremities
Skin
Neurological Exam
- Bio Chemistry
- Pathology
- Microbiology
- Hematology
- Miscellaneous
Sodium: 136 meq/L( normal 135-145 meq/L)
Potassium: 4 meq/L (normal 3.5-5.0 meq/L)
Chloride: 100 meq/L(normal 96-108 meq/L)
Bicarb: 26 meq/L(normal 22-30 meq/L)
Magnesium: 1.9 mg/dl ( normal 1.7 to 2.2 mg/dL )
Phos.: 2.9mg/dl ( normal 2.8 to 4.5 mg/dL)
Bun: 22mg/dl ( normal 6-23 mg/dL)
Creat: 1.1 mg/dl ( normal 0.7 -1.3 mg/dL)
Liver Enzymes - SGOT/AST: 32U/L ( normal 1-35 )
SGPT/ ALT: 43U/L ( normal 1-45 )
GGT: 6 U/L ( normal 8-38 )
Direct Bilirubin: 0.2 mg/dl ( normal 0.1-0.3 )
Total Bilirubin: 1 mg/dl ( normal 0.1 - 1.2 )
NA
NO GROWTH - BLOOD OR URINE
Hemoglobin: 10.2 g/dl ( normal 13.9 -16.3)
Hematocrit: 34% ( normal 42-52 % )
White Count: 11.5 ( normal 4,500 to 11,000 WBCs per microliter) 73 PERCENT NEUTRO
Platelets: 160 ( normal 150,000 to 450,000 platelets per microliter)
Differential: 73 % NEUTROPHILS
CRP : 66 MG/ L - HIGH
- CT Scan
- Xray
- MRI
- Ultrasound
- Echo
- Endoscopic
- Miscellaneous
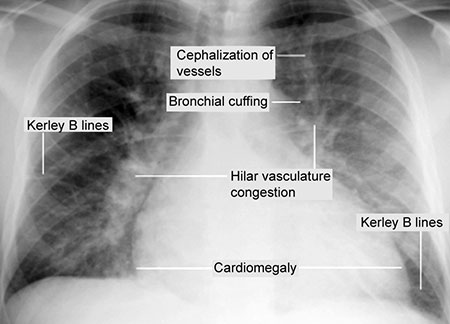
CARDIOMEGALY, HILAR VASCULAR CONGESTION
NA
NA
MITRAL REGURGITATION ON ECHO
SUBCUTANEOUS NODULE ON HAND

Suggested case questions to create interactive quiz. please create questions choices with explanations
1. what is the differntial diagnosis of this case ? ( atleast 4 recommended ) . give alteast 4 plausible choices with one right answer and explanation for each choice.
A.
B.
C.
D,
2. What is the next step that will help in diagnosis of this case ? give alteast 4 plausible choices with right answer and explanation for each choice.
A.
B.
C.
D.
3. What are the management and therapeutic options for this case ? give alteast 4 plausible choices with right answer and explanation for each choice.
A.
B.
C.
D.
The major sequel of acute rheumatic fever is chronic valvular heart disease. Antibodies against streptococcal polysaccharide (carbohydrate cell wall) crossreact with cardiac tissues (myosin and laminin) to cause valve damage by molecular mimicry. During the acute stage, the mitral valve leaflets are inflamed resulting in a diastolic Carey-Coomb’s murmur. Later on, due to smouldering disease, the valves are chronically damaged. Mitral stenosis, aortic regurgitation, mitral regurgitation and aortic stenosis, follow in that order of decreasing incidence.
A migratory or “fleeting” type of polyarthritis with fever and extreme weakness is the commonest manifestation of rheumatic fever. The arthritis typically involves the medium-sized joints such as the elbows, ankles and wrists. Chorea is usually observed in young children as an isolated entity, with rheumatic heart disease occuring a few days later. Erythema marginatum, which is hardly seen, is a pink rash on the trunk which blanches on pressure and is neither painful nor indurated. Rheumatic carditis is a pancarditis. Endocarditis manifests as a new murmur due to inflamed valve leaflets. Myocarditis presents as newly developed myocardial dysfunction. Evidence of pericarditis is a pericardial friction rub or presence of an effusion.
The major sequel of acute rheumatic fever is chronic valvular heart disease. Antibodies against streptococcal polysaccharide (carbohydrate cell wall) crossreact with cardiac tissues (myosin and laminin) to cause valve damage by molecular mimicry. During the acute stage, the mitral valve leaflets are inflamed resulting in a diastolic Carey-Coomb’s murmur. Later on, due to smouldering disease, the valves are chronically damaged. Mitral stenosis, aortic regurgitation, mitral regurgitation and aortic stenosis, follow in that order of decreasing incidence.